With the recent revelation of American rapper, Kanye West, being diagnosed with Bipolar Disorder, the condition has been brought into the spotlight. The term ‘Bipolar’ (meaning “two poles”) signifies the polar opposites of emotional highs and lows. As the name suggests, Bipolar Disorder is characterised by episodic, extreme mood swings in which the individual experiences intense mania and severe depression. Formerly known as ‘Manic-depressive Illness’, the disorder is a fairly common, yet serious mental health condition.
For individuals struggling with the disorder, manic episodes can last days to weeks and are often associated with hyperactivity, an irritable mood, rapid thoughts, increased recklessness, or an exaggerated sense of self-esteem and power. On the other hand, a depressive episode can last weeks to months. In this phase, individuals may experience increased restlessness, a loss of interest in activities (including those that they usually enjoy), poor concentration or disrupted sleep patterns. In more severe cases, these people may also possess suicidal thoughts and behaviours.
In order to help us better understand the condition, we interviewed Deborah Seah, a peer support specialist at Psaltcare.
Deborah started experiencing extreme mood swings in her early primary school years. Having known that her paternal family had a history of mental illness, she identified that her condition was most likely to be genetic. However, she had chosen to suffer in silence until 2 decades later, when she sought psychiatric help for postnatal depression and work-related burnout. At that point, she was diagnosed with Bipolar Disorder as well as Generalised Anxiety Disorder. For Deborah, the disorder reigned control over her life – straining her relationships with her loved ones. Before her diagnosis, others could not understand why she was being so unpredictable, and her erratic behaviour had unfortunately caused numerous misunderstandings.
“It was very challenging to manage my mood swings at the tender age of 8,” she shared. “When I was experiencing my highs, I would talk very fast, have tremendous amounts of energy, get very excited, or become easily irritable and agitated. On the other hand, when I was experiencing my lows, I would feel very sad and experience low energy levels. I could cry for hours or days over trivial matters and be even suicidal at times. The experience of dealing with bipolar disorder consisted of feelings of helplessness, hopelessness and loneliness as I could not predict or control my emotions and energy.” Deborah’s experience with bipolar disorder led her to face an identity crisis – being confused over her contrasting “personalities”, and not knowing which was the real her.
Just like any other mental condition, there are bound to be misconceptions of the Bipolar Disorder, especially if people don’t open up and address it. One such misconception is that individuals struggling with Bipolar Disorder are incapable of managing their mood swings. However, Deborah takes this as an opportunity to debunk such a sentiment: “After a certain point in time, I’ve arrived at a higher level of self-awareness towards my early warning signs, and it has enabled me to gain self-mastery over my condition. When my mood or energy level starts to dip, I’m aware of what could effectively help me to increase my mood and energy. When my mood or energy level is overly high, I know that I need to be extra mindful of not going into overdrive.”
While on the road to recovery, Deborah made a commendable effort in helping herself cope with the disorder. This included reading up on the condition proactively to ensure that she could better achieve self-mastery. Of course, finding a silver lining and staying positive is essential over the course of recovery. Keeping up with articles on others’ success stories and breakthroughs helped her to stay hopeful and confident that recovery is not impossible.
Being highly motivated to make headway towards recovery, Deborah knew that she needed to make changes to her lifestyle. For starters, Deborah:
ensures that she keeps to a good sleep routine and to have sufficient rest
adopts a healthy lifestyle by having a balanced diet and staying active through exercise
stays in a conducive environment for recovery where all potential triggers are removed as much as possible.
She also notes that her Christian faith has played an essential part. Daily prayer and spiritual devotion helped her to calm her mind and provided her with the much-needed inner peace. However, Deborah stresses that one should not brush aside the idea of peer support or psychiatric intervention. The active use of medications coupled with peer support contributed to the turning point in her recovery, and restored any lost hope when the future was seemingly bleak. Connecting to like-minded peers can help one explore new coping strategies and stay on a personal wellness plan.
“Upon knowing my diagnosis, my family took the initiative to purchase books on Bipolar Disorder to understand my condition better,” Deborah recounted. “My family gave me space when I needed it and continually held hope for me even when I gave up on myself. They didn’t pressurise me to make quick progress on my recovery but assured me that they genuinely only wanted me to be happy and that is all that mattered to them. I was deeply touched by their love and concern for me and felt motivated to work hard on my recovery because I realised that they would always be affected whenever I’m suffering.” Through her experience, Deborah holds a strong belief that the hope and support from her loved ones had an immeasurable, significant impact on her, and encourages those who are also supporting their loved ones with mental conditions to stay hopeful.
As of today, Deborah has made promising progress and is well on her way towards achieving mental wellness. After consistently attending a Recovery and Wellness Sustenance (RWS) Workshop at IMH, Deborah graduated with a certificate of participation. Recognising that she benefited much from the workshop, she returned as a Mentor to co-train the subsequent class of peers. In addition, Deborah also completed a module conducted by the National Council of Social Services (NCSS) and was involved in the facilitation for the 3rd and current 5th batch of Peer Support Specialist (PSS) training. She said, “It gave me confidence and reinforced my own recovery as I pay it forward and encourage my peers in their recovery journey. Moreover, it has equipped me with effective coping skills to deal with my mental health condition and it brought my recovery to a higher level.”
To end off, Deborah hopes to pass on an important message to the readers: “To me, there is no shame to be on psychiatric medication or seeking psychiatric help. Just like how people with diabetic conditions need to be on insulin while some people who are asthmatic need to be on Ventolin, people with psychiatric conditions need to take psychiatric medication too. Resilience in Recovery requires these 3 things: Courage – to embrace the past, Gratitude – for the gifts of the present, and Hope – to make the most of the future. I believe that everyone can recover from a mental health challenge, as long as he or she does not give up hope because I am the Evidence of Recovery myself! Everyone recovers at their own pace, just like every flower blooms in its season – let us hold the hope for our loved ones and for those who are battling mental health challenges by cheering them on and being their source of support to believe that recovery is indeed possible.”
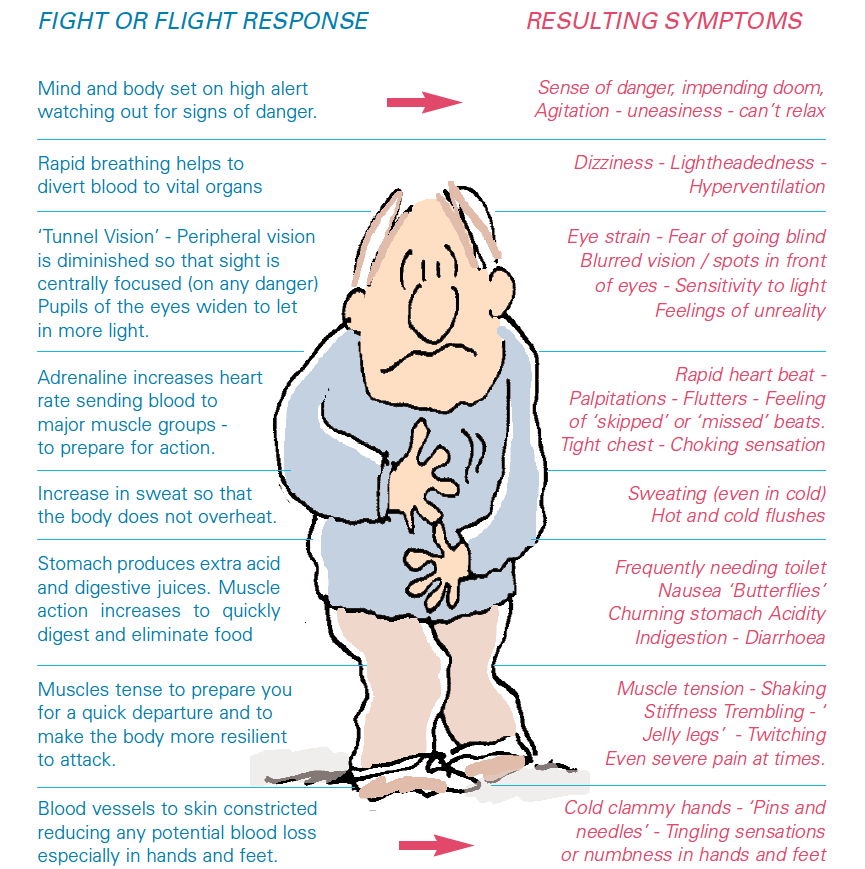
Anxiety refers to a state of anticipation of alarming future events. Anxiety is usually a normal transient response to stress and may be a necessary cue for adaption and coping, the body’s protective mechanism known as the ‘fight or flight response’.
However, anxiety can become pathologic, where it is excessive and inappropriate to the reality of the current situation. It is often described by many as a distressing experience of dread and foreboding.
Anxiety is manifested in the affective, cognitive behavioural and physical domains. The affective states could range from edginess and unease to terror and panic. Cognitively, the experience is one of worry, apprehension and thoughts concerned with emotional or bodily danger. Behaviourally, anxiety triggers a multitude of responses concerned with diminishing or avoiding the distress.
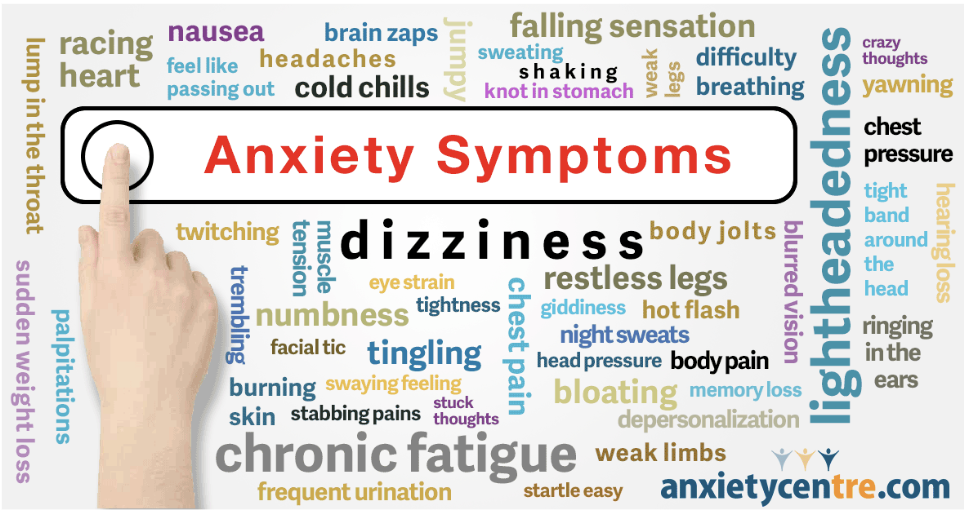
Physical Manifestations of Anxiety
Stimulating the autonomic nervous system results in an array of bodily perturbations.
Several nervous system structures are involved in fear and pathologic anxiety.
The amygdala is responsible for initiating the fight-or-flight response. When activated, the amygdala triggers a series of changes in brain chemicals and hormones that puts the entire body in anxiety mode.
Left untreated, over time the affected individual’s body physically responds more frequently and intensely to worries. Co-morbid depression often sets in. One’s ability to meaningfully function academically, occupationally and socially gets hampered, leading to a deterioration in the quality of life.
Treatment of Pathologic Anxiety
The first point of contact for many patients would be their general practitioners or even the hospital Accident & Emergency department. It is important to evaluate and rule out underlying medical illnesses that may mimic an anxiety disorder, such as thyroid disorders, heart rhythm disturbances, gastrointestinal diseases or alcohol withdrawal. The doctor may order some basic investigations, such as a thyroid function blood test or an electrocardiogram (to check one’s heart rhythm). Once medical causes have been excluded or identified and treated, persisting anxiety symptoms would warrant a psychiatric consultation.
A prescription of anti-depressants such as Selective Serotonin Re-Uptake Inhibitors (SSRIs) to aid in the balancing of the brain neurotransmitters may be suggested. Anxiolytics such as benzodiazepines e.g. Clonazepam may be used in the initial phase of treatment, and thereafter only short courses are prescribed to reduce the risk of dependency.
Cognitive-Behavioural Therapy (CBT) involves cognitive restructuring and anxiety symptom management. Cognitive interventions are aimed at challenging and correcting the inaccurate and maladaptive thought patterns that maintain anxiety disorders. Symptom management techniques e.g. relaxation and breathing re-training procedures, help to eliminate anxiogenic bodily reactions.
Lifestyle adjustments to one’s hectic pace of life need to be made to break the vicious cycle of stress and worry. Developing a healthy routine with regularly scheduled self-esteem-raising activities, ensuring adequate rest and nutrition as well as maintaining social connections are pivotal for mental wellness.
References
Massachusetts General Hospital, Handbook of General Hospital Psychiatry, seventh edition, chapter 13: Anxious Patients.
Both bipolar disorder and schizophrenia were considered severe mental illnesses with no recovery in the past. This is not true in modern psychiatry as we have developed more effective treatments such as medications (psycho-pharmacology) and psycho-social interventions (psycho-therapy and psycho-social rehabilitation) which help patients improve their quality of life as well as reduce symptoms and restore function.
Bipolar disorder and schizophrenia may have similar symptoms which are disturbances in thinking, feelings and behaviour. The major difference is that bipolar disorder is classified as a mood disorder whereas schizophrenia is classified as a psychotic disorder. Mental healthcare professionals make diagnoses based on reports of patients, caregivers, or other information sources as well as observations made during the assessment interview.
Experts have also formulated that schizophrenia and bipolar disorder may be a spectrum disorder with schizophrenia on one end and bipolar disorder on the other end with schizoaffective disorder in the middle of the spectrum.
What is more important however is not the exact diagnosis alone but rather the identification of symptoms so that treatment can be effectively targeted at the relief of the symptoms, restoring function and improving quality of life. This targeted symptom approach has proven to be one of the most effective ways of helping persons recover from these brain conditions.
Let’s discuss some of the common symptoms –
Delusions, which are untrue, unshakable, and unshared beliefs which can exist in both brain conditions.
For example, delusions of persecution which are beliefs of being targeted, being followed, being sabotaged (persecutory) are common in schizophrenia while delusions of grandiosity such as believing that they are particularly important persons and have special powers or ability to save the world (grandiose delusions) are more common in bipolar disorder. For persons with schizoaffective disorder, they might have both persecutory and grandiose delusions at the same time. It also has an underlying co-occurring mood disorder.
Hallucinations which are perceptual disturbances such as hearing voices which are not heard by others, seeing, smelling, tasting or feeling things which are not present are more likely to happen in schizophrenia.
Severe mood swings and manic episodes where the person has fast speech and high energy levels are associated with abnormal spending, socialising, exercising, or expanding businesses with the need for very little sleep over a few days and weeks are more likely to happen in bipolar disorder.
More than half a century ago, most persons suffering from these brain conditions were isolated and confined to asylums as there were no effective treatments until the discovery of medications that can change brain chemistry. Neurotransmitters which are chemicals responsible for brain and other bodily functions were discovered. Noradrenaline, serotonin, and dopamine disturbances were more likely causes in bipolar disorder while dopamine imbalance was a more probable cause of schizophrenia. See https://dana.org/article/neurotransmitters/
The Help Of Modern Medicine
Modern psychopharmacology offers an array of medications which can act on various neurotransmitter sites in the brain. Several medications and several rounds of adjustment and fine-tuning may often be needed to achieve stabilisation with medications with relief of symptoms. This is best done collaboratively with the patient, psychiatrist, and caregiver at the consultation with all the medications brought in for review.
Adjusting to a new medication through an effective therapeutic trial may take at least 2 weeks, starting with the lowest dose and increasing dosing to a maximised symptom relief dose over 2 months.
Medications need to be taken daily to be effective, and this is best done using a pill box and with supervision from a loved one. Medications are served by nurses in the inpatient hospital setting who ensure that the correct dose is directly observed to be taken by the patient – however, this is often lacking in the outpatient setting leading to the return of the symptoms causing distress and dysfunction.
Bipolar & Schizophrenia Treatment Methods
Comparing bipolar disorder and schizophrenia to other brain conditions may be helpful in understanding how one can better achieve remission and recovery.
Epilepsy is a brain condition where there are electrical firing of neurons causing disturbances in thinking, feeling and behaviour. To stay in control of oneself, the doctor may recommend various combinations of anti-epileptic medications to prevent another seizure. In fact, the model of kindling in epilepsy has been used to understand mental health treatment in this highly readable resource essay –https://aeon.co/essays/should-the-kindling-concept-direct-mental-health-treatment
If you speak to someone with experience with epilepsy, they will tell you about ‘warning signs’ and the ‘confusional state’ after a breakthrough seizure.
Similarly, for those struggling with bipolar disorder and schizophrenia, one becomes more aware of ‘warning signs’, and ‘confusional states’ through direct feedback from loved ones who are observant and psycho-educated by healthcare professionals. Charting, monitoring and sharing your experience are key to success in achieving remission and recovery. Use this mood chart and share it with your mental healthcare professionals for more in-depth analysis –https://loricalabresemd.com/wp-content/uploads/2017/12/Personalized-Mood_Chart.pdf
Symptoms management starts with monitoring your symptoms and the response to the treatment – what makes it better, what makes it worse, whether it is mild, moderate or severe. The frequency, intensity and severity can be charted so that effective treatment of psycho-pharmacology (active use of medications) and psycho-social interventions (psycho-therapy and psycho-social rehabilitation) can be targeted to achieve the best outcome for you.
Recovery Is Possible
Your mental healthcare professional can coach and pace you so that it will not be overwhelming. Recovery starts with taking it one day at a time. Be gentle with yourself. Learn to trust and entrust your healing to people who care about you. Learning from feedback as well as charting, monitoring and sharing your experience with loved ones – trusted family or friends or co-workers greatly enhance effectiveness.
Atomic habits by James Clear is an excellent book which illustrates the importance of charting, monitoring and shaping your habits, on the premise of improving 1% daily leading to more than 365% improvement in one year. This is Youtube illustrates how that can happen – “How to become 37.78 times better at anything”.
There are many services available at Promises Healthcare and Community Partners which can help reduce symptoms, restore function, and improve quality of life. Recovery is possible and becomes a reality with appropriate support and adequate skill training. With the right help and support, persons in recovery can live meaningful and satisfying lives.
Here are some real stories that illustrate many facets of mental health and recovery:
Distinguished Professor of Psychiatry Robert Paul Liberman talking about his Bipolar Disorder diagnosis and treatment and his life work on psycho-social rehabilitation
Principles of Transcranial Magnetic Stimulation (TMS)
In the 1800s, world-renowned English physicist Michael Faraday discovered the principles of electromagnetic induction. Fast forward to the 21st century, Faraday’s discovery was harnessed into the clinical practice of transcranial magnetic stimulation (TMS) for the treatment of mood disorders. Based on Faraday’s Law, TMS can stimulate brain neuronal circuits with tiny electrical currents induced by a changing magnetic field.
In Singapore, the practical application of TMS is employed in the form of repetitive transcranial magnetic stimulation (rTMS). In rTMS, magnetic pulses are delivered in trains at specific frequencies. “Fast” (high frequency e.g. 10Hz) stimulation increases cortical excitability for the treatment of depression. Whereas “slow” (low frequency e.g. 1Hz) stimulation reduces cortical excitability for treating anxiety disorders. Furthermore, TMS can be targeted at focused regions of the cortex for superior precision treatment of specific conditions e.g. rTMS at 1Hz to the right orbitofrontal cortex (OFC) reduces intrusive obsessions in obsessive-compulsive disorder (OCD).
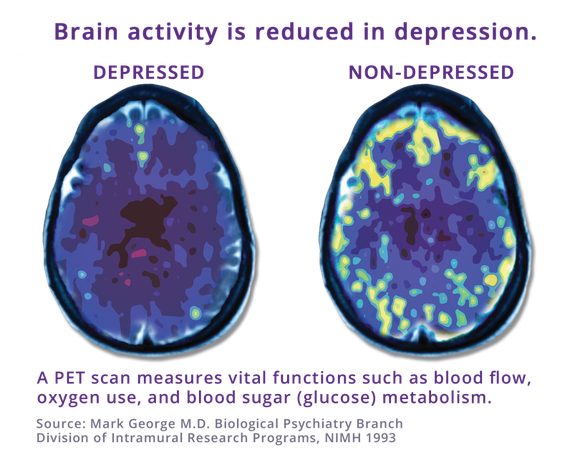
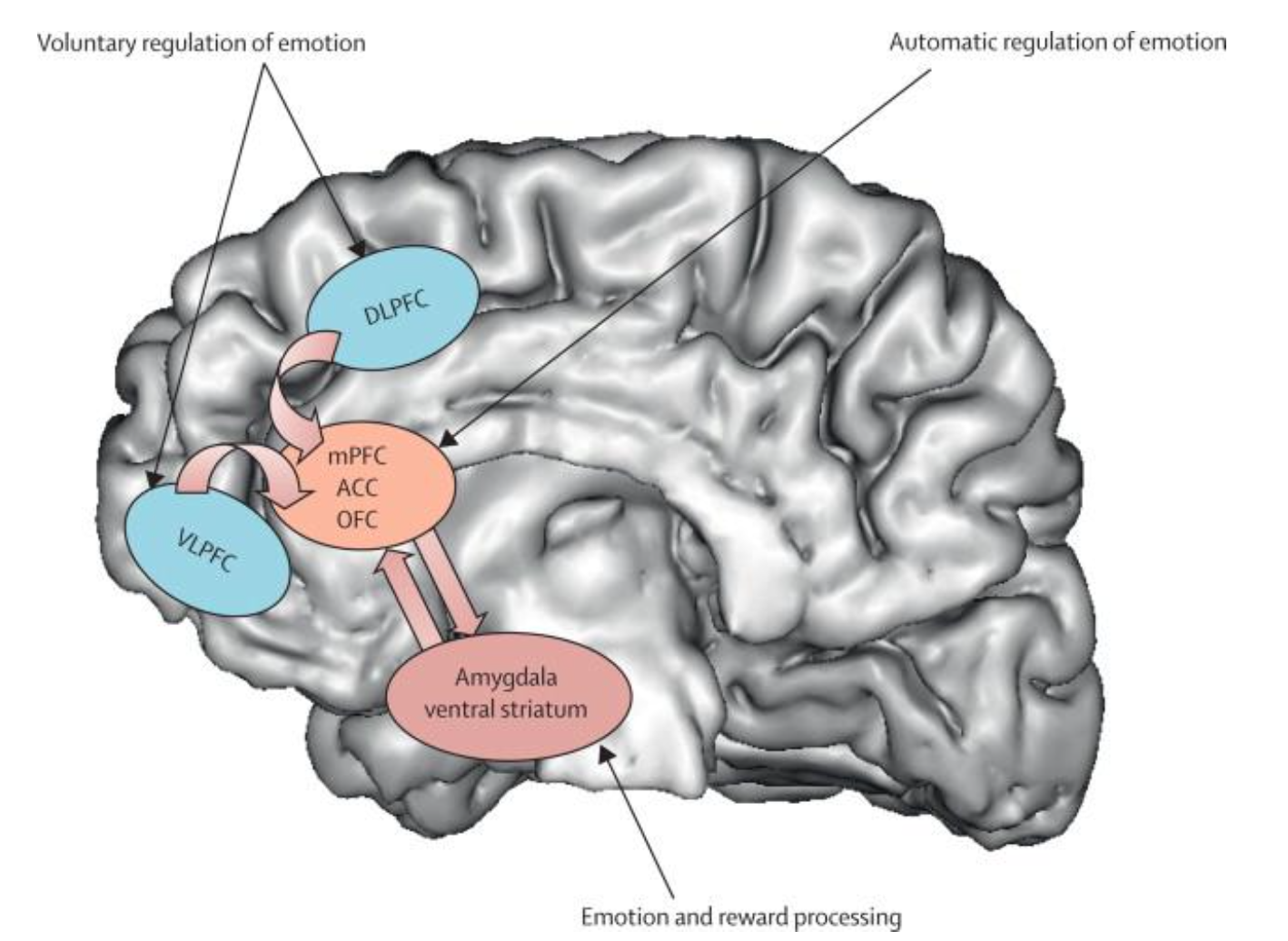
Mood disturbances such as depression are increasingly understood as disorders of connectivity in neural networks linking cortical and subcortical grey structures of the brain. Functional brain imaging has shown dysfunction in cortical regions such as the dorsolateral prefrontal cortex (DLPFC) and anterior cingulate cortex (ACC), as well as deep grey matter structures including the amygdala, nucleus accumbens, hippocampus and hypothalamus. These brain circuits are pivotal for executive functioning, regulation of emotions, reward processing and preservation of memory and cognition. They also link the nervous system to the endocrine system, which mediates the body’s response to stress.
Neuroplasticity and TMS
Evidence suggests that TMS induces neuroplastic changes in these circuits. Neuroplasticity is the ability of the brain to reorganize itself by forming new neural connections. TMS helps readjust neurotransmitter (e.g. serotonin and dopamine) levels in a variety of brain regions. TMS also appears to exert a neuroprotective effect on the brain. Research has shown that TMS decreases brain inflammatory factors reducing oxidative stress on the brain. TMS also boosts the levels of brain-derived neurotrophic factor (BDNF), encouraging neuronal growth in regions such as the hippocampus which is vital for learning and memory. It is postulated that the anti-depressant properties of TMS may also help in normalizing the body’s neuroendocrine stress response system.
rTMS has achieved its place on international treatment guidelines as an augmentation treatment modality to be strongly considered in treatment-resistant depression. It is reported that 30-40% of depressed patients may have inadequate responses to anti-depressant medication treatment. The direct neuronal effects of rTMS may explain why rTMS may work for this group of patients.
rTMS for OCD Treatment and other neurological disorders
In May 2022, the U.S. Food and Drug Administration (FDA) approved the use of the NeuroStar TMS system as an adjunct for treating adult patients suffering from OCD. Promising research is ongoing for the clinical application of TMS in treating Post-Traumatic Stress Disorder (PTSD), addictions, chronic pain, insomnia and many other neurological disorders.
TMS and recovery
With further advancements in TMS research and the incorporation of TMS in routine clinical practice, there is strong hope for recovery and the regaining of optimal functioning for patients afflicted by complex neuropsychiatric conditions.
References
1) Transcranial Magnetic Stimulation
Clinical Applications for Psychiatric Practice
2018 American Psychiatric Association Publishing, First Edition
2) The Science of Transcranial Magnetic Stimulation
William M. Sauvé, MD; and Lawrence J. Crowther, Meng
Psychiatric Annals, Vol44, No.6, 2014
3) Repetitive transcranial magnetic stimulation increases serum brain-derived neurotrophic factor and decreases interleukin-1b and tumour necrosis factor-a in elderly patients with refractory depression
CNN Digital spoke with Dr Jacob Rajesh to give his views regarding a case that shocked the nation of Japan where a teenage girl was stabbed to death by her elderly grandfather.
Here’s his quote:
Jacob Rajesh, a senior forensic psychiatrist at the Promises Healthcare facility in Singapore, said in cases of rapidly progressing Alzheimer’s “it will be difficult to provide an accurate account of what actually happened.”
“There is also the question of fitness to stand trial – is a person fit enough to give evidence on the stand and plead guilty or not guilty?” he said.
Crimes involving dementia patients are also extremely complex, experts said.
In these trying times, mental health is on many people’s minds! While therapy in Singapore has become more accepted, some people still feel trepidation when it comes to psychiatric medication for depression and antidepressants. They also want to know more about side effects and new treatments like Transcranial Magnetic Stimulation (TMS). DR JACOB RAJESH from Promises Healthcare shares his view on all of these things.
What are some commonly used psychiatric medications?
Depression is a very common disorder, affecting between five to ten percent of people, so we use antidepressants quite often. The medications we’ve been using for the past 25 years are called Selective Serotonin Reuptake Inhibitors (SSRIs). These newer generation drugs have much fewer side effects than those used in the past.
They do have some side effects though, the most common being gastric distress, nausea, headaches and insomnia. Some people also report sexual dysfunction and decreased libido. However, these side effects can be managed once the medication and dose is adjusted. SSRIs are usually more tolerated than older antidepressants.
Another group of drugs is the antipsychotics, which are used to treat schizophrenia and bipolar disorders. The second generation antipsychotics have fewer side effects than older ones, along with fewer cognitive effects and extrapyramidal side effects such as causing tremors or stiffness. However, side effects such as weight gain, increased blood sugar and increased cholesterol can occur with some of these drugs; these side effects need to be screened for on a regular basis
Is psychiatric medication an alternative to therapy? Or do they work hand in hand?
Medication and therapy usually work hand in hand. Being medication-compliant is another important part of the mental health recovery treatment as it helps bring stabilisation to the chemical and biological changes in the sufferer that cause the disorder.
For depression, we prescribe medication for moderate or severe symptoms if it’s causing impairment or distress. We also recommend psychotherapy in its various forms: cognitive behavioural therapy, dialectical behaviour therapy, acceptance and commitment therapy, interpersonal therapy or family therapy, depending on the psychosocial stressors.
For bipolar disorder or psychotic conditions like schizophrenia, medications are the mainstays of treatment. However, psychotherapy methods can also help with regulating emotions and give handles to help regulate distorted thoughts when mild symptoms occur. Psychological therapy also plays a role for Obsessive-Compulsive Disorder (OCD) and eating disorders. Here, psychotherapy has a much more important role.
What are some of the misconceptions people have about psychiatric medication?
The most common misconception is that all psychiatric medications make you feel like a zombie – you can’t function, you can’t go to work, your mental faculties are affected. While some of the older generation antipsychotic medications can cause mental fogginess, there are newer ones with fewer side effects. Some people also believe that if they start taking medication, they might become addicted. It is usually the benzodiazepine class of drugs that are addictive in the long term; antidepressants aren’t addictive in the long term. We also see many patients who’ve been taking medication on a long-term basis, but we work with them to minimise side effects. We do this by adjusting the dosage, changing the class of drugs used and lifestyle modification. It’s also worth mentioning that psychologists cannot prescribe any of these drugs, only psychiatrists can.
Can you tell us more about new techniques like Transcranial Magnetic Stimulation?
Transcranial Magnetic Stimulation (TMS) uses electromagnetic waves to stimulate the brain. Unlike electroconvulsive therapy, which is more for people with severe psychotic depression, TMS doesn’t require any sedation. The patient simply sits in a chair and has a device placed at specific parts of the brain where it sends small electromagnetic waves. It is an outpatient procedure and there aren’t usually any side effects.
TMS is used primarily for people with depression who haven’t responded to antidepressants or have severe side effects from medication. It’s not usually a first-line procedure.
Is it as effective as antidepressants?
It works in combination with them. If that alone isn’t helping, TMS can augment the medication. It can also help by itself, but once the treatment stops the patient can relapse, so it’s better to take medication along with it.
What are some psychiatric issues that people may not realise they have?
Many people don’t realise that depression or anxiety disorders are mental illnesses. They think it’s a weakness in their own personality or the result of external stressors they can’t handle. The stigma of mental disorders also plays a big part. People tend to be quick to seek help for physical issues but still feel uncomfortable seeing a psychiatrist. I think it’s becoming more accepted though. There’s a misconception that psychiatrists just provide medication.
What else do they do?
Psychiatrists work in teams. The team-based approach is very important because we have psychiatrists who are qualified doctors along with psychologists who are trained in psychotherapy. We also have social workers, case managers and occupational therapists.
It’s a misconception that psychiatrists cannot do therapy. There are many psychiatrists who are trained in many forms of therapy, but the psychologists are the professionals who study these critical areas in depth. We refer the patients to them because it is their area of expertise.
What would you tell someone who is unsure about seeking help?
Don’t be ashamed of your symptoms or be self-critical. Many feel their symptoms stem from a weak personality or an inability to handle stress. People need to understand that mental health issues can occur for people who’ve done everything right – people with a good job, a good family life, good support and no financial issues. Depression is a biological response and it can happen without any external stressors so there is no shame in seeking help.
Dr Rajesh is a Senior Consultant Psychiatrist at Promises Healthcare, a provider that offers a wide range of psychiatric and psychological services for patients of all ages. Promises is also the only private centre in Singapore to offer Transcranial Magnetic Stimulation.
For more information on psychiatric medication and treatments offered by Promises Healthcare, click here. #09-22/23 Novena Medical Center | 6397 7309
Dinesh is a seasoned writer and editor with seven years of experience covering travel, restaurants and bars. His interests include film photography, cheesy 90s monster flicks, and scouring the island for under-the-radar craft beer bars.
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.Ok