*Visions is an addictions arm of Promises and we help assist clients in Singapore to enable them to improve their lives; and our website provides the images, names, languages, qualifications, and experience of specialists who can help.
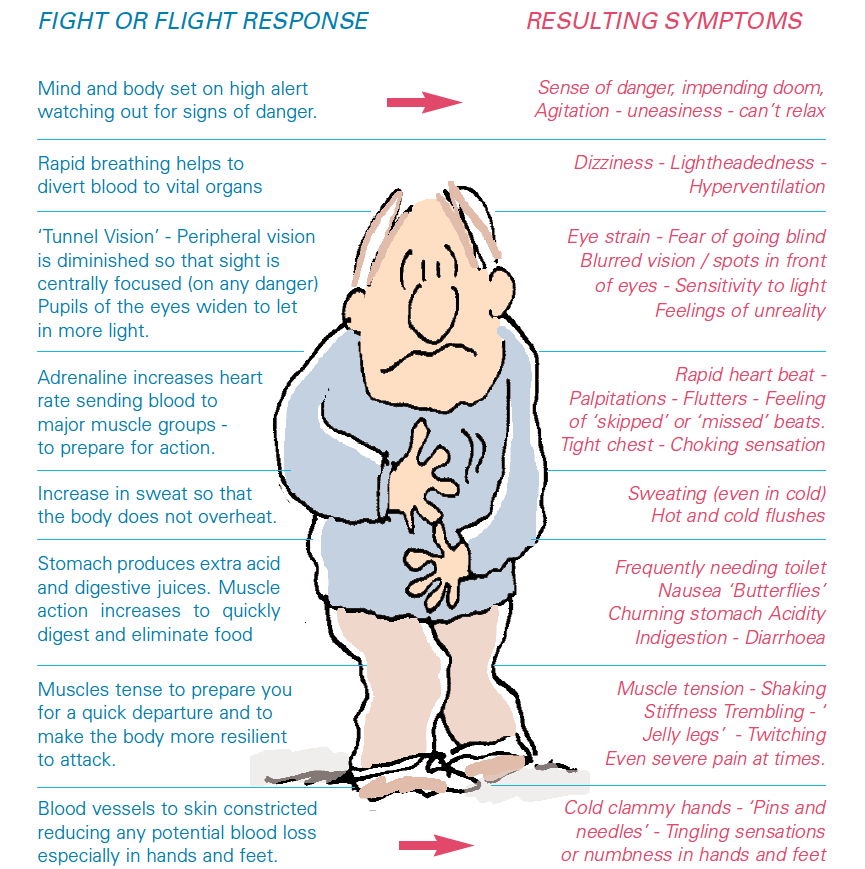
Anxiety refers to a state of anticipation of alarming future events. Anxiety is usually a normal transient response to stress and may be a necessary cue for adaption and coping, the body’s protective mechanism known as the ‘fight or flight response’.
However, anxiety can become pathologic, where it is excessive and inappropriate to the reality of the current situation. It is often described by many as a distressing experience of dread and foreboding.
Anxiety is manifested in the affective, cognitive behavioural and physical domains. The affective states could range from edginess and unease to terror and panic. Cognitively, the experience is one of worry, apprehension and thoughts concerned with emotional or bodily danger. Behaviourally, anxiety triggers a multitude of responses concerned with diminishing or avoiding the distress.
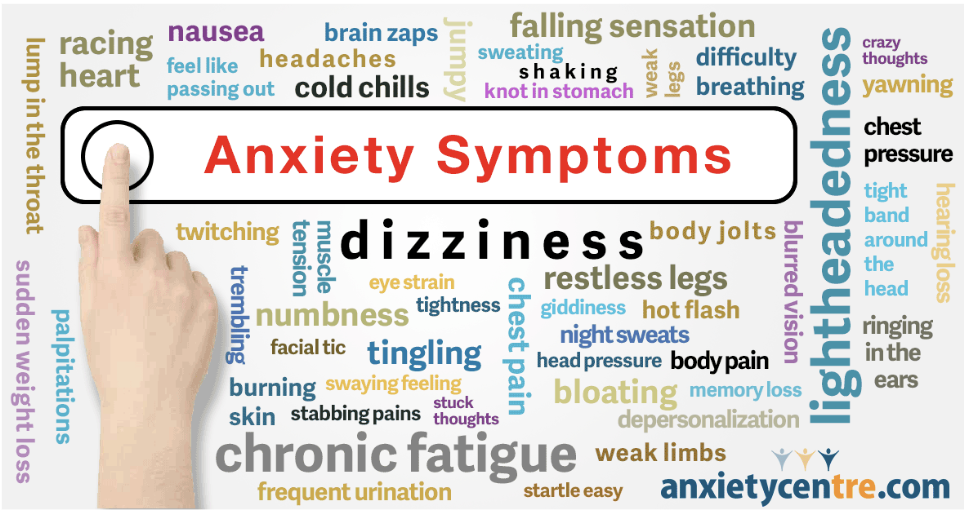
Physical Manifestations of Anxiety
Stimulating the autonomic nervous system results in an array of bodily perturbations.
Several nervous system structures are involved in fear and pathologic anxiety.
The amygdala is responsible for initiating the fight-or-flight response. When activated, the amygdala triggers a series of changes in brain chemicals and hormones that puts the entire body in anxiety mode.
Left untreated, over time the affected individual’s body physically responds more frequently and intensely to worries. Co-morbid depression often sets in. One’s ability to meaningfully function academically, occupationally and socially gets hampered, leading to a deterioration in the quality of life.
Treatment of Pathologic Anxiety
The first point of contact for many patients would be their general practitioners or even the hospital Accident & Emergency department. It is important to evaluate and rule out underlying medical illnesses that may mimic an anxiety disorder, such as thyroid disorders, heart rhythm disturbances, gastrointestinal diseases or alcohol withdrawal. The doctor may order some basic investigations, such as a thyroid function blood test or an electrocardiogram (to check one’s heart rhythm). Once medical causes have been excluded or identified and treated, persisting anxiety symptoms would warrant a psychiatric consultation.
A prescription of anti-depressants such as Selective Serotonin Re-Uptake Inhibitors (SSRIs) to aid in the balancing of the brain neurotransmitters may be suggested. Anxiolytics such as benzodiazepines e.g. Clonazepam may be used in the initial phase of treatment, and thereafter only short courses are prescribed to reduce the risk of dependency.
Cognitive-Behavioural Therapy (CBT) involves cognitive restructuring and anxiety symptom management. Cognitive interventions are aimed at challenging and correcting the inaccurate and maladaptive thought patterns that maintain anxiety disorders. Symptom management techniques e.g. relaxation and breathing re-training procedures, help to eliminate anxiogenic bodily reactions.
Lifestyle adjustments to one’s hectic pace of life need to be made to break the vicious cycle of stress and worry. Developing a healthy routine with regularly scheduled self-esteem-raising activities, ensuring adequate rest and nutrition as well as maintaining social connections are pivotal for mental wellness.
References
Massachusetts General Hospital, Handbook of General Hospital Psychiatry, seventh edition, chapter 13: Anxious Patients.
Senior Clinical Psychologist, Henny Tan, was interviewed by the popular YA YouTube channel, LadiesFirstTv (Titan Digital Media) about the stigma a person might face when being identified as having a mental illness.
Click on the red play button to watch this 13min 24 sec video.
Most of us look forward to the festive season. After all “‘tis the season to be jolly”. It is a time for family and friends to be gathered together, often with the accompaniment of special treats and food. However, this may not always be the case for individuals who struggle with eating disorders.
Across various cultures, food is a unifying cultural thread, and eating is a huge and important part of our social lives. Oftentimes we forget the pervasiveness of food in our everyday lives. Have you ever considered how integral the role of food is in building social connectedness and relationships? We catch up with friends over meals and have informal business meetings over coffee. We also celebrate important occasions and milestones over food. The phenomenon of foodstagramming (a term used to describe the act of taking pictures of one’s food and posting it on social media), or “the camera eats first”, also dominates our social media.
As a result of the emphasis that is being placed on food, individuals with an eating disorder may feel tremendous stress and anxiety partaking in food-focused family traditions and gatherings with friends during the holiday season.
What are eating disorders?
Eating disorders are a category of psychological conditions that manifest themselves in persistent and unhealthy relationships between body image, food, eating and exercise. They usually develop in adolescence and young adulthood and are often associated with a whole host of distressing thoughts and emotions. Eating disorders can affect people of all ages and of any race, gender or body type.
Some types of eating disorders include:
Anorexia Nervosa
An eating disorder characterised by weight loss (or lack of appropriate weight gain in children), unhealthy eating patterns, intense fear of gaining weight and significant body image concerns. This condition is extremely dangerous as it can lead to malnutrition, starvation, and death.
Bulimia Nervosa
Bulimia is characterised by a cycle of bingeing and purging, where the individual eats large amounts of food (larger than what most people would eat in a similar period of time) in a way that feels out of their control, and then engages in purging which involves self-induced vomiting, fasting, or excessive exercise, Individuals with Bulimia also tend to have significant body image concerns.
Binge-eating Disorder
Binge-eating disorder involves periods of consuming unusually large amounts of food in a discrete period of time, accompanied by a sense of loss of control over eating. Binge-eating episodes are commonly associated with difficult emotions such as guilt, disgust and shame.
Struggles Faced During the Holiday Season
Food
A daily struggle for someone with an eating disorder is worrying about what and how much they will eat, how to burn off the calories consumed. When faced with an abundance of food choices and especially food that they do not commonly eat or labelled as “bad”, such worries become exacerbated. For example, someone with binge-eating urges may find it difficult to control their eating during such situations, leading to increased feelings of guilt and shame, as well as negative beliefs about themselves that come with these feelings.
Disruption of Routines
Obligations to attend various parties and gatherings will also likely disrupt everyday routines such as meal timings and exercise. In addition, structured meal plans that may be essential for someone at a specific stage of eating disorder recovery may also be impacted when dining with others.
Expectations
The holiday season is also a time when we are faced with expectations from family and friends to be happy and relaxed, and to indulge in food. However, for individuals with anorexia nervosa, they may find it extremely difficult to finish their food when family is watching what they eat, or may feel pressured when others are encouraging them to eat larger amounts of food, which can lead to feelings of shame and guilt. Asking someone if they have eaten is often a way of showing we care, but for someone with an eating disorder this could potentially trigger a whole slew of body-image related thoughts. Additionally, stress may also come in the form of worrying about how to manage comments from others about how they look or what they are eating or not eating.
Isolation
Individuals with eating disorders tend to feel isolated as they may withdraw from social gatherings as a way of coping with the deeply rooted fear of being negatively evaluated by others. During the holiday season where gatherings involve many more people, this fear can become intensified. They often find it hard to express their anxieties and struggles to family and friends, while at the same time feel unable to escape such situations, resulting in them feeling overwhelmed and detached.
How One Can Manage The Struggle
Preventive Measures and Coping
Given the challenges that someone with an eating disorder might face during the festive season, it is important to be proactive and plan ahead to make it easier to transition into the holidays. Friends and family can also be a significant source of support.
Plan Ahead
Adhere to a meal plan as much as possible to avoid binge or restrictive eating habits.
Identify potential triggers. List them down and try to brainstorm appropriate solutions or coping for each one of them.
List down coping statements that you think might be helpful. Remind yourself the reasons to leave the eating disorder out of this meal.
Plan non-food related activities that are fun and relaxing to recharge or bond with loved ones. You might feel most vulnerable during the first hour after meals, so plan to do activities that may help to distract yourself from the difficult thoughts or urges to binge or purge.
Arrange check-in sessions to review your game plan with your psychologist before the holiday season.
Practise how to politely set boundaries and prepare a list of topics in case you need to change the topic for when someone makes comments about your appearance or eating that make you feel uncomfortable.
Communicate
Speak with family members or other members of your support system before the holidays to help them understand your needs and potential triggers.
Identify a support person or a “buddy” who can help with sticking to your plans as well as provide emotional support when needed. It might help to arrange a code word or signal to indicate that you are feeling overwhelmed and need additional support.
Self-compassion
Be kind to yourself! Acknowledge that you are stepping outside your comfort zone. It is understandable that this might be difficult and challenging for you, but struggling does not mean you are failing.
Set realistic goals and expectations of yourself. Take things one step at a time.
Catch yourself when you criticise yourself again. Recognise that you are doing the best you can.
Give yourself the gift of enjoying the meal. Remove the idea of treating food as a “reward”, and give yourself permission to enjoy the food and company.
How Family and Loved Ones Can Help
Be there for a loved one who is struggling. Listen to their struggles without making any judgments.
Ask them how they feel and try to validate their feelings, even if you may not fully understand what they are going through.
Avoid being the “food police” unless the treatment team has given you a plan to monitor and portion food for your loved one.
Avoid making comments and judgments about calories, eating and physical appearance.
Refrain from making criticisms and instead offer support and words of encouragement.
Body Dysmorphic Disorder (BDD), in simple terms, is a condition involving an obsessive focus on one or more perceived flaws or defects in appearance. While the perceived flaw may be minor and inconspicuous, individuals struggling with this disorder are inclined to spend a large proportion of their waking hours worrying and finding means to fix these flaws. This includes seeking dermatological or cosmetic procedures and exercising excessively to fix their appearance. Depending on its severity, BDD can be disabling – the emotional distress it causes can affect one’s functioning at social events, work and in the public eye.
BDD is estimated to affect approximately 2 percent of the adolescent and adult population worldwide, and preliminary studies in Singapore have also noted a similar proportion. This figure is, however, likely to be underreported due to the nature of the disorder, where affected individuals are unable to recognise the symptoms of the disorder. Coupled with the lack of awareness of BDD, people associate these BDD symptoms with the “physical flaw” itself.
While there is no definitive cause, there are risk factors that can contribute to the onset of BDD. These can include bullying or abuse, perfectionism, constant competition with others, genetics, and other mental health conditions such as depression, anxiety or obsessive-compulsive disorder (OCD). With the prevalence of social media, this condition is further exacerbated as it perpetuates body image comparison and the image of an “idealised body”. This can trigger such compulsive behaviour in vulnerable individuals, especially if they struggle with low self-esteem. Chemical imbalances can also trigger the onset of BDD in the brain or the use of certain drugs such as ecstasy in susceptible people.
What is the diagnostic criteria for BDD?
For a BDD diagnosis, there is a set of criteria that the individual must meet. According to the Diagnostic Statistical Manual of Mental Disorders (DSM V), they are:
Preoccupation with one or more perceived defects or flaws in physical appearance that are not observable or appear slight to others.
At some point during the course of the disorder, the individual has performed repetitive behaviours (e.g., mirror checking, excessive grooming, skin picking, reassurance seeking) or mental acts (e.g., comparing his or her appearance with that of others) in response to the appearance concerns.
The preoccupation causes clinically significant distress or impairment in social, occupational or other areas of functioning.
The appearance preoccupation is not better explained by concerns with body fat or weight in an individual whose symptoms meet diagnostic criteria for an eating disorder.
In addition, the individual would need to be assessed on their degree of insight regarding body dysmorphic disorder beliefs. In other words, how convinced are they that their bodies look “deformed” or “ugly”? A person with good or fair insight recognises that these beliefs are definitely or probably false. A person with poor insight would think that these beliefs are probably true. In the worst-case scenario, a person with absent insight or delusional beliefs would be completely convinced that their body dysmorphic beliefs are true.
What forms of treatment are available for BDD?
A combination of psychotherapy and pharmacotherapy is often implemented in the treatment plan for BDD. Cognitive Behavioural Therapy (CBT) is a psychotherapeutic method which aims to help one recognise maladaptive thought and behaviour patterns, and teach self-help coping strategies that can improve one’s quality of life. CBT has been proven to be an essential form of treatment for other mental health conditions as well, including depression and anxiety disorders. CBT for body dysmorphia would focus on helping the patient build self-esteem, and learn to tolerate the distress of “exposing” their perceived defects to others. It helps them manage their concerns with healthier coping mechanisms instead of taking extreme measures to fix their appearance. This includes training them to cope with symptoms of anxiety.
Medication is sometimes used in combination with CBT for maximum efficacy. One common medication used to relieve BDD symptoms include antidepressant medications. Selective Serotonin Inhibitors (SSRIs) in particular, can ease and reduce compulsivity, as well as overwhelming symptoms of anxiety or depression.
You may wonder why we don’t proceed with cosmetic or surgical procedures to correct their perceived flaws, especially if they seek such measures. As mentioned, BDD often involves flawed beliefs surrounding an inconspicuous or minor flaw in appearance. We must acknowledge that any medical or surgical procedure carries health risks, regardless of the extent of the surgery. Any unnecessary alterations or body modifications may not only lead to undesirable health effects but may also lead to dissatisfaction with the results. Should the surgical procedure not turn out as expected, this could worsen the patient’s BDD.
We use cookies to ensure that we give you the best experience on our website. If you continue to use this site we will assume that you are happy with it.Ok